Breaking Down Barriers: The Compassionate Service of Leg Washing
A Conversation with Jonathan Rout
Project Officer, Church’s Auxiliary for Social Action (CASA), India
David Addiss: Jonathan, it is wonderful to be with you to discuss your work in India with CASA, the Church’s Auxiliary for Social Action. Your work has focused on training people within villages how to provide care and treatment – such as leg and foot washing – for people with lymphedema – a painful, deforming, and stigmatizing condition caused by lymphatic filariasis (LF). How did you get started?
 Jonathan: I joined CASA as a village level community organizer after I completed my Master’s degree in social work and my law degree. In 2003, with the support of IMA World Health, we started a pilot project on LF focused mainly on health education and awareness for the community. Prior to our program, a person had died in this area during a campaign to provide diethylcarbamazine (DEC), the medication for LF. It had been argued in court that DEC had caused the death, and the local people were nervous about taking the medication, which is needed to stop the transmission of LF. We felt that if we offered the proper health education then maybe people would again accept taking DEC tablets. DEC doesn’t help with managing lymphedema, but it is an important first step to stop the spread of the disease.
Jonathan: I joined CASA as a village level community organizer after I completed my Master’s degree in social work and my law degree. In 2003, with the support of IMA World Health, we started a pilot project on LF focused mainly on health education and awareness for the community. Prior to our program, a person had died in this area during a campaign to provide diethylcarbamazine (DEC), the medication for LF. It had been argued in court that DEC had caused the death, and the local people were nervous about taking the medication, which is needed to stop the transmission of LF. We felt that if we offered the proper health education then maybe people would again accept taking DEC tablets. DEC doesn’t help with managing lymphedema, but it is an important first step to stop the spread of the disease.
 Every day we went into the field and tried to educate the people. We selected young boys and girls from each village and gave them proper training on how to educate their community. There were three main topics: why LF exists, what it is, and how to prevent it. We used mass media, educational materials, and street theater to create awareness and educate them about LF. We taught them how to identify persons who have microfilaria in their blood. We earned the confidence of the people. We tested their blood in the night when the microfilaria are active and gave them the medicine. These activities were well-received, and the people began to demand that we distribute DEC tablets. With the support of the state government, we started a mass drug administration (MDA) program in the district. We went house-to-house distributing water and biscuits along with the medicine. The program was so successful that the same community where the person had died all took the DEC.
Every day we went into the field and tried to educate the people. We selected young boys and girls from each village and gave them proper training on how to educate their community. There were three main topics: why LF exists, what it is, and how to prevent it. We used mass media, educational materials, and street theater to create awareness and educate them about LF. We taught them how to identify persons who have microfilaria in their blood. We earned the confidence of the people. We tested their blood in the night when the microfilaria are active and gave them the medicine. These activities were well-received, and the people began to demand that we distribute DEC tablets. With the support of the state government, we started a mass drug administration (MDA) program in the district. We went house-to-house distributing water and biscuits along with the medicine. The program was so successful that the same community where the person had died all took the DEC.
David: How did the leg washing program evolve?
Jonathan: Slowly we took responsibility for one block, then one district, and then gradually one district with more than 185,000 families. I was coordinator for the entire program. When I learned about LF morbidity management I jumped into that activity. Without any hesitation, I was trained by Dr. Shenoy and Dr. LeAnne Fox and began the leg washing programs in 2005.
 Doctors from the local hospitals suggested that we must use gloves when washing the legs of patients. But for me the gloves created a barrier between the patient and me. I needed to touch the patient, to have body-to-body contact. LF is not a contagious disease so we continued washing with our bare hands. Our patients became very emotional and cried when we touched them. They told us that no one had ever touched their feet in a caring manner; rather, they were usually shunned and kept out of sight due to shame from their families.
Doctors from the local hospitals suggested that we must use gloves when washing the legs of patients. But for me the gloves created a barrier between the patient and me. I needed to touch the patient, to have body-to-body contact. LF is not a contagious disease so we continued washing with our bare hands. Our patients became very emotional and cried when we touched them. They told us that no one had ever touched their feet in a caring manner; rather, they were usually shunned and kept out of sight due to shame from their families.
Orissa has a strong caste system and our volunteers come from all castes and religions. Some volunteers come from the higher caste, while the patients are usually from an underprivileged group. The volunteers from the higher caste are so moved by seeing the impact of washing feet that they forget about their caste, their religion, and they join the foot washing team. Foot washing helps to break down barriers in the community. It also encourages the health workers at the village level to touch patients rather than just give advice. Through this effort, those that have lymphedema are now going to the temples, sitting in the marketplaces, and engaging in mainstream society. They are accepted by their families and the community. This gives me great satisfaction.
David: You’ve not mentioned the word compassion yet, but what you are describing sounds a lot like compassion. What is the role of compassion in your work and in your life?
 Jonathan: After a year of working at CASA, I met a high-level government officer in Jharkhand state that knew about my work. He asked me, “What is your background?” When I told him he said, “That is not a job for you. You have an education, a law degree. Leave this job and go back to Orissa and search for a better job.” He demotivated me in such a manner that for two days I was disturbed and thought that I have to leave this job. I went back to my home and talked to my father. He told me, “I have not disclosed a very secret thing about your life. When you were at the age of six months, you were affected by cholera, severe diarrhea. At the hospital bed, you were so sick that we lost our hope. I and your mother prayed that if you survived, we would dedicate you for the service of God. That was our intention. In your job now, you are dedicating yourself to service of the people. That is the work of God, to support the unprivileged people, the hungry people, the diseased people. Go and do this work that gives you such satisfaction.” That was my turning point. I think this is God’s plan for me and nobody can block the way. I receive spiritual satisfaction when I clean the legs of the patients. This is the compassionate work of Jesus.
Jonathan: After a year of working at CASA, I met a high-level government officer in Jharkhand state that knew about my work. He asked me, “What is your background?” When I told him he said, “That is not a job for you. You have an education, a law degree. Leave this job and go back to Orissa and search for a better job.” He demotivated me in such a manner that for two days I was disturbed and thought that I have to leave this job. I went back to my home and talked to my father. He told me, “I have not disclosed a very secret thing about your life. When you were at the age of six months, you were affected by cholera, severe diarrhea. At the hospital bed, you were so sick that we lost our hope. I and your mother prayed that if you survived, we would dedicate you for the service of God. That was our intention. In your job now, you are dedicating yourself to service of the people. That is the work of God, to support the unprivileged people, the hungry people, the diseased people. Go and do this work that gives you such satisfaction.” That was my turning point. I think this is God’s plan for me and nobody can block the way. I receive spiritual satisfaction when I clean the legs of the patients. This is the compassionate work of Jesus.
 You showed compassion, David, by initiating the foot-care management program. You informed us about the patients who were hidden within homes, how to identify them, and how to support them so that their life would be better and less painful. Since 2005 we have covered 2,300 villages and directly touched and provided care to 24,730 patients. We hope to reach 60,000 more lymphedema patients. We have also identified 1131 people with hand swelling, 126 people with breast swelling, and 6148 people with hydrocele in our program area.
You showed compassion, David, by initiating the foot-care management program. You informed us about the patients who were hidden within homes, how to identify them, and how to support them so that their life would be better and less painful. Since 2005 we have covered 2,300 villages and directly touched and provided care to 24,730 patients. We hope to reach 60,000 more lymphedema patients. We have also identified 1131 people with hand swelling, 126 people with breast swelling, and 6148 people with hydrocele in our program area.
David: What are some of the challenges you have faced and overcome?
Jonathan: There are three main challenges to the morbidity management work. The first challenge is social: families are still hiding the patients. The second is vested interest groups in some of the villages: they sometimes want to claim that they are behind CASA but we are doing this work on our own. The third is financial. We would like to reach 60,000 patients and provide them three things – two towels, four soaps, and two ointments – and we need more money to do this. Of all the challenges, the social stigma is the most difficult to overcome.
David: CASA is a Christian organization, and yet you work with people of other faiths. How do you bring people of different faiths together?
Jonathan: I am the only Christian in the LF program unit at CASA. My colleagues are Hindus and Muslims. They are the health workers, the supervisors, the coordinators, and the volunteers. In the 2,300 villages where we work, two or three of these villages are Christian. All others are Hindu and Muslim villages. In some places, they are nervous that our agenda may be to convert them to Christianity but they soon realize and see for themselves that is not the case.

We never say anything about religion. Instead, we conduct the training programs in a general meeting place in the village where everyone can see. We explain what is CASA, how CASA is working, and why we are in the village. We address all the doubts in that meeting and invite questions from the village people. We tell them that our program is for one year with just one leg care kit and that the village boys and girls will give training to their parents, to their grandparents. It is not CASA who will go to their house.
What I realized is that if you are doing good work and people experience that, then they will support it. In many places where we conduct our programs the work goes very late into the night. Hindu and Muslim families bring food to us and give us a room to sleep. This way we have very good experiences.
David: CASA has a very strong commitment to both compassionate action and social justice. How are these two things – compassion and justice – related?
Jonathan: When patients are crying and suffering on the bed, our first responsibility is to relieve them from their pain rather than talk about social justice. After the foot-care management they are better and they are happy. Then we can attend to justice.
 We are now doing advocacy work to see what benefits the government can give to the patients. They are citizens of this bright country and have rights to receive benefits, but they are not able to get to the hospitals because of their deformities. If a patient who developed lymphedema was the breadwinner for the family, with their deformity they are not able to do anything. It is not only that the family is hungry; the entire family unit has collapsed. The government supports programs for citizens with tuberculosis and with HIV. Why not offer support to people with lymphatic filariasis morbidity? These patients are citizens, they are paying taxes, and they have every right to receive support. At the very least the government could provide soap, towels, and ointment at subsidy rates for each patient.
We are now doing advocacy work to see what benefits the government can give to the patients. They are citizens of this bright country and have rights to receive benefits, but they are not able to get to the hospitals because of their deformities. If a patient who developed lymphedema was the breadwinner for the family, with their deformity they are not able to do anything. It is not only that the family is hungry; the entire family unit has collapsed. The government supports programs for citizens with tuberculosis and with HIV. Why not offer support to people with lymphatic filariasis morbidity? These patients are citizens, they are paying taxes, and they have every right to receive support. At the very least the government could provide soap, towels, and ointment at subsidy rates for each patient.
David: What thoughts or recommendations do you have for young people who are thinking about global health or filariasis as a career?
 Jonathan: Even if the MDA is successful at stopping LF transmission today, we have another 20 to 25 years of responsibility to help patients with LF morbidity. This is not just the case in Orissa; it is all over the world, wherever lymphatic filariasis patients are living. You and Mr. Paul Derstine and Dr. LeAnne Fox came from such a far distance to help our patients. It is now our responsibility to look after our families, friends, and neighbors. I am thankful to Dr. Sushant Agrawal, my Director, for his continued support. Even though I am now in a different program area with CASA, whenever I have time I am visiting the villages on my own. I am washing feet and interacting with the patients. Responding to the pains of our people should be part of our culture. Young people need to join the effort. Caring for others gives spiritual pleasure.
Jonathan: Even if the MDA is successful at stopping LF transmission today, we have another 20 to 25 years of responsibility to help patients with LF morbidity. This is not just the case in Orissa; it is all over the world, wherever lymphatic filariasis patients are living. You and Mr. Paul Derstine and Dr. LeAnne Fox came from such a far distance to help our patients. It is now our responsibility to look after our families, friends, and neighbors. I am thankful to Dr. Sushant Agrawal, my Director, for his continued support. Even though I am now in a different program area with CASA, whenever I have time I am visiting the villages on my own. I am washing feet and interacting with the patients. Responding to the pains of our people should be part of our culture. Young people need to join the effort. Caring for others gives spiritual pleasure.
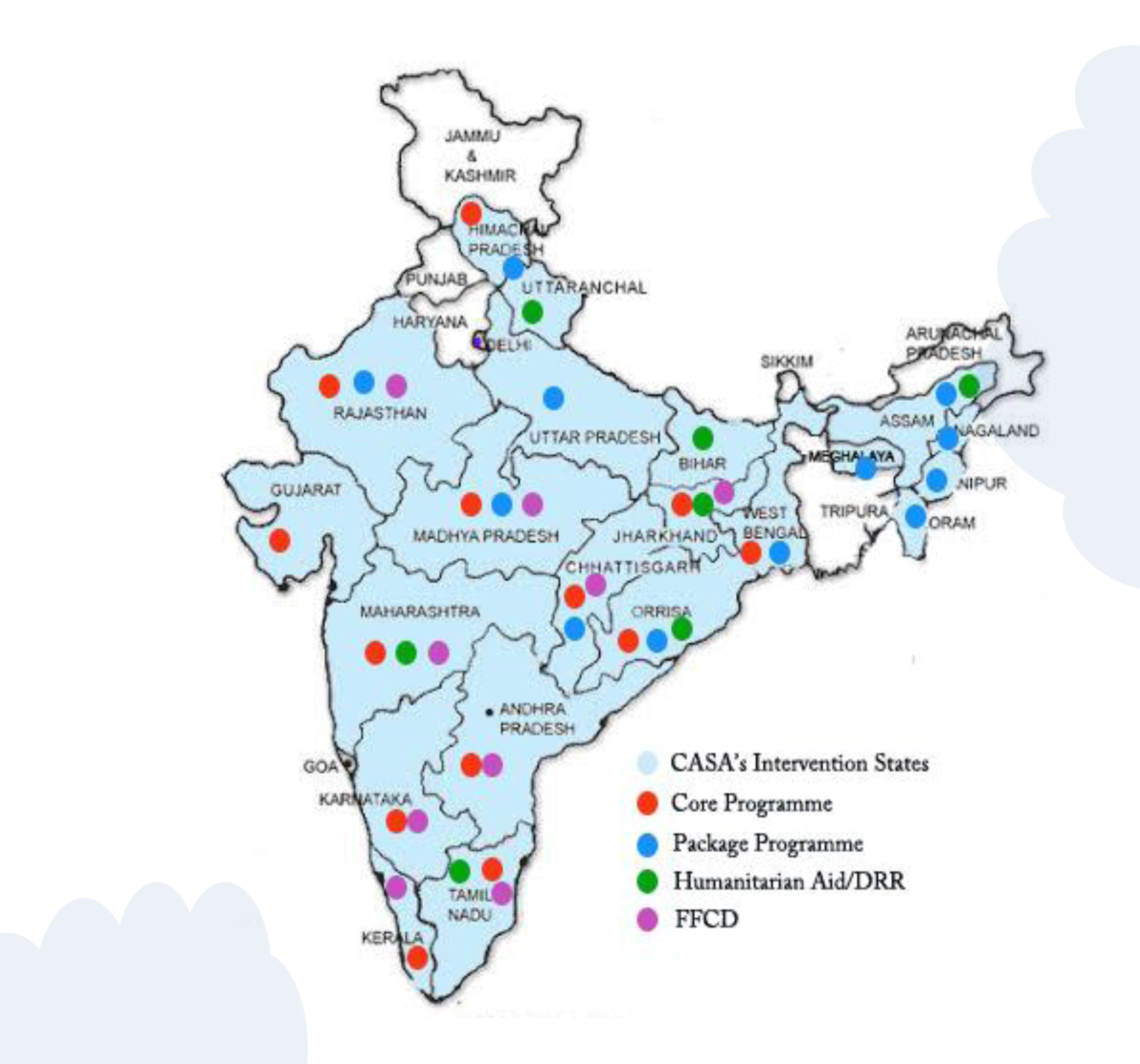
 Mr. Jonathan Rout is Project Officer for Church’s Auxiliary for Social Action (CASA), India. CASA is a premier relief and development organization in the country, acting as the outreach arm of 24 Protestant and Orthodox Churches in India. Its primary objective today is to strengthen the poor and promote the efforts of marginalized groups of the Indian society towards sustainable development leading to social justice and self-sufficiency. While CASA is a Christian organization constituted and supported by the Churches, its outlook is secular and it is mandated by the Indian Protestant and Orthodox Churches to carry out its interventions irrespective of religious, ethnic, caste or political considerations.
Mr. Jonathan Rout is Project Officer for Church’s Auxiliary for Social Action (CASA), India. CASA is a premier relief and development organization in the country, acting as the outreach arm of 24 Protestant and Orthodox Churches in India. Its primary objective today is to strengthen the poor and promote the efforts of marginalized groups of the Indian society towards sustainable development leading to social justice and self-sufficiency. While CASA is a Christian organization constituted and supported by the Churches, its outlook is secular and it is mandated by the Indian Protestant and Orthodox Churches to carry out its interventions irrespective of religious, ethnic, caste or political considerations.